See also: IRC log
<ericP> scribenick: MikeDenny
<ericP> ericP: blah blah blah
<ericP> ... and still more blah blah blah
test
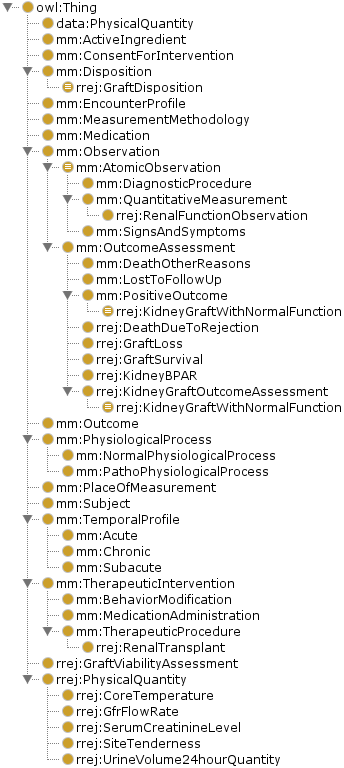
<ericP> FDA TA MetaModel
<kerstin> URL?
<ericP> FDA TA MetaModel
<ericP> Protege
<ericP> FDA Therapeutic Areas modeling effort underway to describe disease effects -- being supported by HCLS with OWL modeling.
<ericP> bottom-most ontology for use in Protege
<matthias_samwald> just dialed in.
<ericP> FDA TA MetaModel
<matthias_samwald> thanks.
<ericP> May be helpful for efficacy assessment with notion of 'therapeutic intervention' class.
<Sajjad_INSERM> You mentioned that you facing some errors: are they parsing errors or modelling errors?
<emory> speaking in above where attributed to ericP
<emory> Answers question about lack of fine granularity in model by referring to it as a metamodel that will drive specific therapeuic areas.
<kerstin> I can see some future alignment opportunties with some of the mid-level OBO ontologies e.g. Ontology for General Medical Science (OGMS) and Ontology for Biomedical Investigations (OBI)
<emory> Answers question about kinds of observations supported like composite observations by asking for suggestions.
< ??> Suggests nested panels etc.
<emory> Question of level of detail needed in this modeling is still being discussed with FDA.
<emory> IIn response to question about clinical trial submission using OWL specification instead of FHIR, for example, this is taken as a consideration.
<kerstin> If for example neurological TA is one of the 12 FDA TAs it could be interesting to look into some alignement opportunties with the NeuroPsychological Testing Ontology https://code.google.com/p/neuropsychological-testing-ontology/
<??> How do you handle disease where you do not know underlying physiological process?
<emory> The metamodel is now a pragmatic approach.
<kerstin> MikeDenny: Good question - check out my references above and also the reference articla behind OGMS, check out http://code.google.com/p/ogms/
<emory> Ansers question of how do you link this metamodel with other standards by referring to C-CDA and FHIR mapping being a goal of the project.
<kerstin> quick question - How are behind folks behind MikeDenny and TallTed alias (behind kerstin in Kerstin Forsberg, AstraZenenca)?
<kerstin> thx
<emory> Calls for volunteers to continue on this work to demonstrate to FDA the value of RDF and OWL modeling.
<eafry> http://64.87.15.66:8888/webprotege
<ericP> eafry: neda took the UMLS data and created a script to dump the hierarchy in the current SNOMED disease tree
<ericP> ... there may be other relevant branches but to start, she grabbed the disease tree
<ericP> ... she exposed the preferred label as the node label
<ericP> ... her next pass will expose the UMLS CUI and the SNOMED code
<ericP> ... the purpose of the tree is to make available the majority of the disease concepts in SNOMED
<eafry> The login for the site above showing a couple of public ontologies will need username + password of 'test'.
<ericP> ... it's very disorganized
<ericP> ... a goal is to find a smaller set of terms which can be post-coordinated to submsume current pre-coordinated terms
<ericP> ... once we get the extracts with the UMLS codes, we can start extend into other ontologies
<ericP> ... so we've been thinking about axes needed for post-coordination
<eafry> Show relation between pre-coordination and post-coordination SNOMED coding to express diseases using an OWL model.
<ericP> ... age, etiology (which could go into the TA metamodel), signs and symptoms, ...
<ericP> ... enable q's like "what are the diseases which produce hives and shortness of breath?"
<ericP> ... there's a discussion area, as well as notes and viersion history
<ericP> ... this will ideally allow us to collaboratively move to post-coordinated
<ericP> neda: when we have these concepts as classes, we'll be able to attach more rules and use them for e.g. clinical decision support
<eafry> The site includes a Disease Ontology and a FHIR Ontology.
<ericP> Sajjad_INSERM: what branches of SNOMED do you have?
<ericP> eafry: |clinical observations| |disease|
<ericP> ... we'll need more stuff, but that's our start
<eafry> The Disease Ontology is the branch of SNOMED starting at Clinical Obervations - Disease.
<ericP> 1 Document different ways that terminology mappings led to inappropriate assertions, potentially because of transitive inference as in Hong Sun's examples.
<ericP> 2 Examine successful/valid uses of termmaps for sensitivity to use context. Does your use of the termmap imply that it's useful to someone else?
<ericP> 3 Describe how to fix the failures, e.g. the lenses from EHR4CR.
<ericP> 4 Codify the context associated with the fixes to enable someone else with the same context to employ them.
<ericP> 5 Once we have a good story, ask the owners of the terminologies to own the mappings.
<kerstin> Lenses are from OpenPHACTS
<ericP> alister: the idea of a Lense is you turn on or off mapping because e.g. two chemicals share stereochemistry or INCHI key
<kerstin> Some examples of Justifuications sitting behind the Open PHACTS Lenses are described in my blog post on applying the same thinking on terminiligy mappings http://kerfors.blogspot.se/2013/09/justifications-of-mappings.html
<ericP> ... the tool captures the mappings and justifications
<Alister> Lens used in Terminology Mapping to turn on and off mappings based on their context.
<agray> Here is the paper where we outline the original idea behind lenses. This was done in the context of linking data instances rather than terminologies, but the approach could easily be ported across. http://ceur-ws.org/Vol-951/paper5.pdf
<ericP> Call for volunteers to continue work on this Terminology Mapping project.
<agray> I'm happy to be involved.
<allister> In response to request, will try to dig up a demo that works.
<kerstin> Here's a nice blog post from Hong et al in the SALUS project http://www.srdc.com.tr/projects/salus/blog/?p=241
<agray> I will email details of a working example for the use of lenses in the Open PHACTS project. (It needs some explanations to make it work.)
<Sajjad_INSERM> Paper Link on Terminology Mapping from Hong: http://arxiv.org/ftp/arxiv/papers/1310/1310.4156.pdf
<ericP> next meeting 7 Jan
Good Bye!
This is scribe.perl Revision: 1.138 of Date: 2013-04-25 13:59:11 Check for newer version at http://dev.w3.org/cvsweb/~checkout~/2002/scribe/ Guessing input format: RRSAgent_Text_Format (score 1.00) Found ScribeNick: MikeDenny Inferring Scribes: MikeDenny WARNING: No "Present: ... " found! Possibly Present: Claude EmoryFry IPcaller Kerstin_Forsberg MikeDenny Mike_Denny P10 P14 P2 Sajjad_INSERM aaaa agray alister eafry ericP inserted kerstin kerstin_ matthias_samwald neda scribenick You can indicate people for the Present list like this: <dbooth> Present: dbooth jonathan mary <dbooth> Present+ amy WARNING: No meeting title found! You should specify the meeting title like this: <dbooth> Meeting: Weekly Baking Club Meeting WARNING: No meeting chair found! You should specify the meeting chair like this: <dbooth> Chair: dbooth Got date from IRC log name: 17 Dec 2013 Guessing minutes URL: http://www.w3.org/2013/12/17-hcls-minutes.html People with action items: WARNING: Input appears to use implicit continuation lines. You may need the "-implicitContinuations" option.[End of scribe.perl diagnostic output]
{kind=link}